Student: A lot of dust on this Dyspnea diagram. Where did you get it?
Professor: The schematic diagram I got from a very old backup disk of manuscripts written in the early 1990s. Notice that the diagram is an attempt to place uncomfortable subjective qualities, i.e., symptoms, for breathing into a hierarchy as shown below:
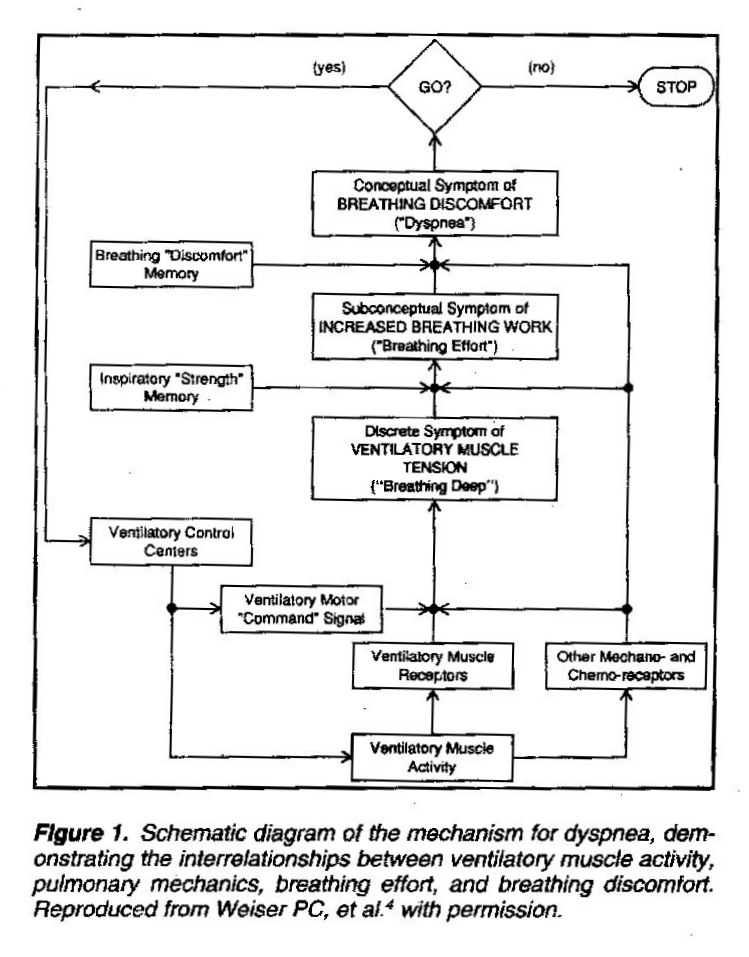
Dyspnea Model 1992
Student: Hmm. From the top down, the hierarchy seems to be:
- Conceptual Symptom of BREATHING DISCOMFORT (“Dyspnea”)
- Subconceptual Symptom of INSCREASED BREATHING WORK (“Breathing Effort”)
- Discrete Symptom of VENTILITORY MUSCLE TENSION (“Breathing Deep”)
Professor: After the hierarchy was constructed, then a possible feedforward-feedback set for physiological loops were added (Weiser & Henson, 1992; Weiser, Mahler et al., 1993), with the emphasis on interrelationships among:
- ventilatory muscle activity
- as assessed by mechanoreceptor feedback of increased ventilatory muscle tension and integrated as Breathing Deep with
- the comparison to the activity of collaterals for the Ventilatory Motor Command Signal(s),
- pulmonary mechanics work / effort
- by various receptors sensing increased breathing work and integrating it as Breathing Effort with
- the comparison to Inspiratory “Strength” Memory, and
- breathing discomfort
- by various cortical areas sensing and integrating interoreception as Dyspnea with
- the comparison to Breathing “Discomfort” Memory.
Student: Looks to me that your description had anticipated the discussion of Work / Effort subjective qualities published in: An American Thoracic Society Statement: Update on the Mechanisms … of Dyspnea 2012.
Professor: Now I have downloaded several relevant articles for their section on Work / Effort.
Student: I wonder how these articles expand on this schematic diagram.
Professor: Well, I got sidetracked on cluster analysis of the subjective qualities of dyspnea. I was attempting to:
- relate the findings of various studies done in the last 15 years to
- our 1970s analysis of end-of-exercise intensities of reported subjective qualities.
Take Home Message: The subjective qualities of dyspnea appear to be neuroanatomically organized into a hierarchical manner.
Next: The cluster analysis of the subjective qualities of dyspnea will be published on review page of this website, and the subjective qualities of Work / Effort as well as Tightness and Air Hunger / Insufficient Inhalation will be part three of the Dyspnea posts.
References
Parshall MB, Manning HL, Bourbeau J, Calverley PM, Gift AG, Harver A, Lareau SC, Mahler DA, Meek PM, O’Donnell DE. (2012) An official American Thoracic Society statement: Update on the mechanisms, assessment, and management of dyspnea. Am J Resp Crit Care 185: 435-452.
Weiser PC, Henson DM. (1992) Mechanisms of Exertional Dyspnea in Patients with Chronic Heart Failure. Heart Failure 8:202-209.
Weiser PC, Mahler DA, Ryan KP, Hill KL, Greenspon LW. (1993) Clinical assessment and management of dyspnea. In: Pulmonary rehabilitation: Guidelines to success. 2nd edition. Hodgkin, J, Bell CW, eds. Philadelphia: Lippincott, 478-511.